| disease | Temporal Space Infection |
Temporal space infection refers to an acute suppurative infection in the temporal space, with the main clinical manifestations being swelling confined to the temporal region or accompanied by extensive swelling in areas such as the masseteric-parotid region, cheek, orbital region, and zygomatic region.
bubble_chart Etiology
The temporal space is located in the temporal region above the zygomatic arch and is divided by the temporalis muscle into the superficial and deep temporal spaces. It communicates with the infratemporal space, pterygomandibular space, masseteric space, and buccal space along fatty connective tissue (Figure 3).
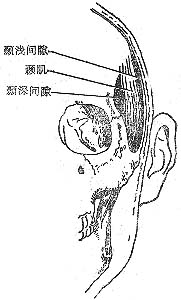
Figure 3 Anatomical location of the temporal space
Infections of the temporal space often result from the spread of infections in the masseteric space, pterygomandibular space, infratemporal space, or buccal space. Otogenic infections (such as suppurative otitis media or temporal mastoiditis), boils or carbuncles in the temporal region, and secondary infections following temporal injuries may initially involve the temporal space.
bubble_chart Clinical Manifestations
The clinical manifestations of temporal space infection depend on whether it is a simple temporal space infection or accompanied by infection of adjacent multiple spaces. Therefore, the swelling may be limited to the temporal region alone or involve extensive swelling in areas such as the parotid-masseteric region, cheek, orbit, and zygomatic region. The affected area exhibits pitting edema, tenderness, mastication pain, and varying degrees of trismus. Fluctuation can be palpated in superficial temporal space abscesses, whereas deep temporal space abscesses require aspiration of pus for confirmation.
The temporalis muscle is thick and the temporal fascia is dense, making it difficult for deep abscesses to rupture spontaneously. Prolonged accumulation of pus on the surface of the temporal bone can lead to osteomyelitis. The squamous part of the temporal bone has thin walls with little diploë between the inner and outer plates. Infection can spread directly through bone sutures or via vessels entering the cerebral membrane, leading to complications such as meningitis and brain abscess.1. Medical History: There may be a history of pericoronitis or periapical periodontitis of the maxillary third molar before the onset of infratemporal space infection. The history of posterior superior alveolar nerve block anesthesia, foramen ovale anesthesia, and infratemporal-trigeminal-sympathetic nerve block should also not be overlooked.
2. Clinical Manifestations: Due to the deep and concealed anatomical location of the abscess, although systemic infectious and toxic symptoms such as high fever, headache, loss of appetite, and elevated white blood cell count are prominent, facial redness and swelling are not very noticeable. Instead, indirect manifestations include significant redness and swelling at the mucosal fold of the maxillary tubercle on the affected side, swelling and shallowing or bulging of the vestibular groove, obvious tenderness, and fluctuation. Pus can easily be aspirated by puncture at this site. Swelling and tenderness are also present above and below the zygomatic arch and in the upper posterior mandibular region.
bubble_chart Treatment Measures
Temporal space cellulitis secondary to infection of adjacent spaces may subside after incision and drainage of abscesses in other spaces. Once a temporal space abscess forms, incision and drainage should be performed. Different types of incisions are used depending on the depth of the abscess and the size of the cavity: for superficial abscesses, a single skin incision within the temporal hairline may suffice; for deep abscesses, two or more straight incisions parallel to the direction of the temporalis muscle fibers can be made; when temporal bone osteomyelitis is suspected, a curved skin incision can be made along the attachment of the temporalis muscle, cutting through the muscle attachment and elevating the temporalis from the bone surface to fully expose the temporal squama for drainage. When performing a curved incision, it is crucial to avoid making transverse incisions across the muscle fibers on the temporalis, as cutting the temporalis muscle may injure its nerves and blood vessels, impairing its function (Figure 1). In cases of multi-space infection, an additional incision should be made in the submandibular region for through-and-through drainage (Figure 2).
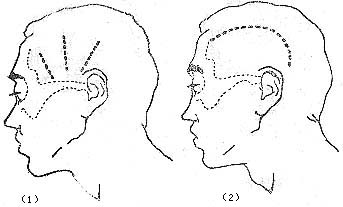
Figure 1 Incisions for drainage of temporal space abscess (1) Straight incision (2) Curved incision
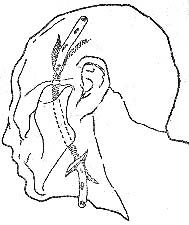
Figure 2 Through-and-through drainage for temporal and infratemporal space abscesses
After incision and drainage of a temporal space abscess, if swelling persists, pus does not decrease, and the bone surface feels rough upon probing, osteomyelitis should be confirmed by X-ray. Active debridement of necrotic bone and infected tissue should then be performed to prevent further intracranial infection.


