| disease | Elbow Joint Tuberculosis |
Subcutaneous nodules of the elbow joint rank first among the three major joints of the upper limb, accounting for 0.92% of subcutaneous nodules in all bones and joints throughout the body. The majority of patients are young adults, with roughly equal distribution between males and females and between left and right sides. Some reports indicate cases where both elbow joints are affected in the same patient. Most patients also have subcutaneous nodules in other organs.
bubble_chart Pathological Changes
The elbow joint structure belongs to the hinge-type joint, composed of three bones: the distal end of the humerus with its two condyles, the proximal end of the ulna with its trochlear notch, and the head of the radius. These form three articular surfaces enclosed within a single joint capsule: the humeroulnar joint, the humeroradial joint, and the proximal radioulnar joint. All three articular surfaces are covered by a thin joint capsule, which is deficient posteriorly and reinforced anteriorly.
The joint is stabilized by strong ligaments and muscles (such as the brachialis, brachioradialis, and extensor carpi radialis longus) to enhance stability.
The primary functions of the joint are flexion and extension of the forearm, as well as pronation and supination of the forearm.
bubble_chart Clinical Manifestations
Subcutaneous tuberculosis of the elbow joint, like other joints, progresses slowly with mild initial symptoms, primarily manifesting as pain, local swelling, tenderness, and limited mobility. Simple bone subcutaneous tuberculosis most commonly occurs in the olecranon of the ulna, followed by the lateral epicondyle of the humerus. Swelling and tenderness are confined to the affected area. Cold abscesses from olecranon subcutaneous tuberculosis are found nearby, while abscesses from lateral malleolus subcutaneous tuberculosis may spread along the extensor muscle spaces to the forearm, forming multiple abscesses. Simple synovial subcutaneous tuberculosis is rare, presenting as swelling around the joint. Grade I swelling first appears in the medial and lateral aspects of the triceps brachii, with the depressions between the medial and lateral epicondyles of the humerus and the olecranon becoming full. Tenderness around the elbow joint is widespread. As the disease progresses to total joint subcutaneous tuberculosis, swelling and tenderness worsen, often resulting in fusiform swelling of the affected limb, with frequent sinus formation from abscesses. Joint mobility becomes further restricted, and severe destruction in total joint subcutaneous tuberculosis may lead to pathological dislocation. When the elbow joint lesion heals, the joint often becomes ankylosed in a non-functional position.
bubble_chart Auxiliary ExaminationPlain X-ray of a simple subcutaneous tuberculous nodule shows localized osteoporosis and soft tissue swelling. In central subcutaneous nodules of the olecranon or lateral malleolus, sequestrum formation may be observed. If the lesion involves the adjacent diaphysis, periosteal new bone formation can be seen. In early-stage total joint subcutaneous tuberculous nodules, localized bone destruction at the joint margins or grade I subchondral bone plate blurring may be present. In advanced-stage total joint subcutaneous tuberculous nodules, there is extensive blurring of the subchondral bone plate and narrowing of the joint space. Secondary infection of the sinus tract shows sclerotic bone changes.
The diagnosis can be easily made based on medical history, clinical manifestations, and X-ray findings.
bubble_chart Treatment Measures
1. For simple synovial or osseous subcutaneous nodules, fix the elbow joint at 90° flexion and the forearm in a neutral rotation position using a Gypsum splint until the muscular rigidity and pain of the elbow joint disappear. Remove the Gypsum splint daily and perform elbow flexion and forearm rotation exercises 2–3 times. For simple osseous subcutaneous nodules, especially those located outside the joint, surgical removal should be performed as early as possible. For simple synovial subcutaneous nodules, intra-articular INH injections can be administered, either between the lateral epicondyle of the humerus and the radial head or between the olecranon of the ulna and the trochlea of the humerus posteriorly.
2. If conservative treatment for synovial subcutaneous nodules or early-stage total joint subcutaneous nodules shows no improvement, surgical intervention may be performed.
(1) Treatment of simple synovial subcutaneous nodules of the elbow joint: Approach the elbow joint posteriorly via an "S"-shaped or straight incision. Reflect the triceps muscle in a tongue-like fashion downward, and at the level of the elbow joint, make incisions toward the medial and lateral epicondyles of the humerus. Subperiosteally detach the common extensor and flexor tendons from the medial and lateral epicondyles to expose the medial and lateral collateral ligaments, the annular ligament of the radius, and the joint capsule. Flex the elbow to 90°, then transect the medial and lateral collateral ligaments, the annular ligament, the joint capsule, and the synovial membrane to enter the elbow joint.Resect the thickened and edematous synovial membrane posterior to the humeroulnar, humeroradial, and proximal radioulnar joints, and curette the granulation tissue at the cartilage margins. Further flex the elbow to approximately 120° and excise the synovial membrane and necrotic tissue anterior to the joint.
Irrigate the area, then suture the transected collateral ligaments, annular ligament, joint capsule, and triceps tendon. Fix with a Gypsum splint for 3 weeks before initiating joint mobility exercises.
(2) Treatment of simple osseous subcutaneous nodules:
For osseous subcutaneous nodules without significant sequestra (central or marginal types) that do not involve the elbow joint, non-surgical treatment is initially attempted. If ineffective, surgical intervention may be performed based on the location of the lesion, using different surgical approaches.
(a) Posterior midline incision of the ulna: After incising the posterior ulnar membrane, perform lesion debridement, then close the wound in layers and immobilize with a Gypsum splint for 3 weeks.
(b) Medial epicondyle incision of the humerus: With the elbow flexed at 90°, make a medial incision extending 4 cm above and below the joint at the apex of the medial epicondyle. Isolate the ulnar nerve in the ulnar groove posterior to the medial epicondyle and retract it posteriorly. Detach all soft tissues anterior to the medial epicondyle, then osteotomize the medial epicondyle with a small chisel and reflect it distally along with the common flexor tendon, taking care to protect the branches of the median nerve entering the flexor muscles at their lateral border. The joint capsule can then be incised to debride the lesion at the medial epicondyle. Note that the median nerve passes anterior to the joint.(c) Lateral epicondyle incision of the humerus: Make a lateral incision extending 4–5 cm above and below the joint at the apex of the lateral epicondyle. Expose the apex of the lateral epicondyle and dissect through the interval between the triceps, extensor carpi radialis longus, and brachioradialis muscles from distal to proximal. Near the proximal end of the incision, take care to identify the radial nerve. Subperiosteally detach the common extensor tendon from the lateral epicondyle and reflect it laterally to expose the humeroradial joint, protecting the deep branch of the radial nerve entering the supinator muscle. Subperiosteally detach the brachioradialis and extensor carpi radialis longus, incise the joint capsule, and expose the lateral aspect of the elbow joint.
(3) Elbow joint forked resection: Suitable for advanced-stage total joint subcutaneous nodules in patients over 12 years old.
Use a posterior approach to the elbow joint. The total resection range of the distal humerus and proximal ulna/radius is 2–4 cm. Resecting too little may impair joint mobility, while excessive resection may compromise the attachment points of the common extensor and flexor tendons, leading to postoperative joint laxity and instability.
Completely excise the radial head but preserve the radial tuberosity where the triceps tendon attaches. Preserve the coronoid process and part of the olecranon on the proximal ulna as attachment points for the brachialis and triceps muscles.
After bone resection, debride any remaining soft tissue lesions, irrigate the wound, and drill two Kirschner wires from the olecranon into the distal humerus in different directions to maintain a 1–1.5 cm gap between the bone ends. Leave the wire ends protruding through the skin for later removal (Figure 1).
Postoperatively, immobilize with a Gypsum splint for 3 weeks.
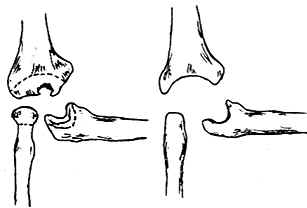
(1) Before Resection (2) After Resection
Figure 1 Elbow Joint Fork Resection
Merge other organs subcutaneous node.


