| disease | Congenital Pseudoarthrosis of the Clavicle |
Congenital pseudarthrosis of the clavicle is a rare deformity, characterized by a visible gap in the middle of the right clavicle at birth. As the child grows, a painless lump develops at the site.
bubble_chart Etiology
Some scholars recently pointed out that on the 7th day of the embryonic cycle, a disruption in the connection between the cartilage centers at both ends of the clavicle leads to pseudarthrosis of the clavicle. The subclavian artery pulse on the right side is positioned higher and closer to the clavicle, increasing pulsatile pressure on the clavicle, which may be the reason for right clavicle involvement. Occasionally, left-sided involvement is observed, which occurs due to dextrocardia with a high-positioned left subclavian artery pulse. Bilateral involvement is caused by bilateral cervical ribs or a high-positioned first rib.
bubble_chart Clinical Manifestations
At birth, swelling in the middle of the clavicle can be observed, with no history of birth trauma. As the child grows older, a painless lump appears locally (Figure 1). Varying degrees of movement can be felt between the two ends of the clavicle, with no tenderness. The sternal end of the clavicle is positioned higher and located anteriorly and medially to the other end. During early childhood, due to the gravitational pull of the upper limb, the lateral part of the clavicle tilts downward, the shoulder joint descends, and mobility at the pseudarthrosis increases. The overlying skin becomes thin and atrophied, the scapular edge protrudes, and the shoulder joint appears asymmetrical. However, shoulder joint movement is generally normal, with only a few patients experiencing limited abduction and weakened arm strength. X-ray images show enlargement and thickening of the two ends at the clavicular pseudarthrosis.
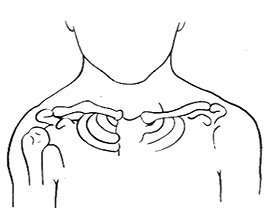
Figure 1 Localized lump on the clavicle
The diagnosis can be easily made based on the presence of a localized mass over the clavicle and findings on X-ray after birth.
bubble_chart Treatment Measures
Owen, Gilson, and Carroll suggest that the optimal age for treating congenital pseudarthrosis of the clavicle is between 3 to 4 years old, while Tachdjian advocates for surgical treatment as early as 1 year old. The surgical procedure includes resection of the pseudarthrosis, internal fixation, and autologous iliac bone grafting.
Key surgical points:
1. Incision: Make a 4-6 cm long curved incision along the skin crease over the clavicle.
2. Resection of pseudarthrosis: Strip the clavicle subperiosteally and expose the pseudarthrosis. Remove the soft tissue, cartilage, and sclerotic bone at the pseudarthrosis site until normal bone tissue is reached.
3. Internal fixation and bone grafting: Use a threaded pin for intramedullary internal fixation, then implant autologous iliac bone fragments into the clavicular defect.
4. Postoperative Velpeau plaster fixation, with the plaster changed every 3 weeks. Shoulder joint exercises can begin after 8-10 weeks of fixation, and the threaded pin can be removed once the bone graft has healed.
At birth, it should be differentiated from obstetric clavicle fracture, which has a history of birth trauma, localized tenderness, pseudoparalysis of the affected limb, and callus formation visible on X-rays to exclude this condition. In childhood, it should be distinguished from acquired clavicular pseudarthrosis, which has a history of trauma, and the slender fracture ends can differentiate it. Additionally, although individuals with cleidocranial dysplasia may have partial or complete absence of the clavicle, they lack pseudarthrosis masses and exhibit skeletal abnormalities in other parts of the body, such as pelvic and limb dysplasia, making it easy to differentiate from this condition.


