| disease | Velopharyngeal Insufficiency |
Velopharyngeal insufficiency is a disorder of pronunciation and swallowing caused by the inability of the velopharynx to close properly due to lesions in the soft palate or pharyngeal wall.
bubble_chart Etiology
Soft palate lesions, such as soft palate paralysis, prevent the soft palate from moving upward and backward to contact the posterior pharyngeal wall; 20-40% of patients after cleft palate repair have incomplete closure; soft palate defects and scar contracture, tumor destruction or surgical removal of part of the soft palate, trauma, subcutaneous node, ulcer, non-specific inflammation, etc., cause scar contracture of the soft palate and lead to this disease. Posterior pharyngeal wall lesions, such as pharyngeal constrictor paralysis, post-adenoid surgery, pharyngeal wall tumors, and inflammatory sexually transmitted disease changes, destroy the pharyngeal wall and prevent it from contracting forward to narrow the pharyngeal cavity, leading to this disease.
bubble_chart Clinical Manifestations
During pronunciation, the inability to close the velopharyngeal port results in open nasal sounds, unclear articulation, and speech disorders. When swallowing, food may reflux into the nasal cavity, especially with liquids. Due to the abnormal opening of the Eustachian tube, symptoms such as ear fullness, a sense of blockage, and hearing loss may occur. Physical examination may reveal scarring or defects in the soft palate, and during the pronunciation of "ah," the soft palate and the posterior pharyngeal wall fail to close.
bubble_chart Treatment Measures
Seek the cause of the disease for corresponding treatment. Soft palate activity training and speech training can increase the movement of the soft palate and are effective for patients with mild symptoms. For patients with obvious scars or significant deficiencies and severe symptoms, surgical treatment such as soft palate lengthening, pharyngoplasty, or palatopharyngeal plasty can be considered. Pharyngoplasty for less severe cases can involve a transverse incision in the posterior pharyngeal wall, blunt dissection, followed by longitudinal suturing. For more severe cases, materials such as fascia, cartilage, bone, or plastic can be inserted under the muscle layer of the posterior pharyngeal wall to elevate it, which can yield better results. Palatopharyngeal ring ligation is a method used in oral surgery to repair cleft palate; it can lengthen the soft palate and reduce the pharyngeal cavity. ① During surgery, a relaxation incision is made between the soft palate and the molars. A dissector is used from the posterior part of one relaxation incision, along the circular fibers of the superior constrictor muscle at the level of the lateral pharyngeal wall, to perform a submuscular dissection towards the lateral pharyngeal wall until reaching the midline of the posterior pharyngeal wall. A ring ligation needle (thread passer) with a No. 7 thread is passed from the posterior part of the relaxation incision along the dissected tunnel to the midline of the posterior pharynx, and one end of the ligation thread is pulled out. ② The same method is used to dissect the tunnel on the other side to the perforation at the midline of the posterior pharyngeal wall, and the ligation thread is pulled out on the other side. Alternatively, after dissecting the tunnels on both sides, the ligation thread can be passed from one relaxation incision to the other in one go. This way, the ligation thread forms a semi-circular shape at the posterior pharyngeal wall. ③ One end of the ligation thread is threaded through a large round needle, passed from one relaxation incision at the level of the palatal aponeurosis near the junction of the hard and soft palate, behind the greater palatine vessels, through the deep layer of the soft palate muscles to the midline, and then to the opposite side, exiting through the opposite relaxation incision. The ligation thread is then tied, reducing the nasopharyngeal cavity to about 1 cm in a circular manner (Figures 1 and 2).
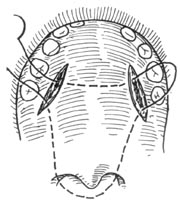
Figure 1 Perforation and ligation
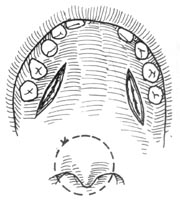
Figure 2 Ring ligation suturing


