| disease | Myocardial Infarction Complicated by Ventricular Septal Rupture |
Ventricular septal rupture is one of the serious complications following acute myocardial infarction. Among cardiac ruptures caused by acute myocardial infarction, those located in the ventricular septum account for about 10%. Pathological autopsy data from fatal cases of acute myocardial infarction show an incidence of ventricular septal rupture ranging from 1.3% to 2.0%. The first case was reported by Latham in 1847, and successful surgical repair was achieved by Cooley in 1957.
bubble_chart Pathological Changes
In cases of ventricular septal rupture, the extent of transmural myocardial infarction is generally extensive. The occurrence of ventricular septal rupture typically happens around 2 weeks after myocardial infarction, with the shortest being 24 hours and the longest being 23 days. The most common site of ventricular septal rupture (60%) is the anterior portion of the ventricular septum, near the apical region, caused by severe stenosis or obstruction of the left anterior descending coronary artery leading to full-thickness infarction of the anterior wall. Rupture in the posterior portion of the ventricular septum accounts for about 20%, resulting from lesions in the posterior descending coronary artery causing inferior wall myocardial infarction. When both the left anterior descending and posterior descending arteries are obstructed due to disease, multiple ruptures may occur in the ventricular septum, appearing sequentially within a few days. Cases of posterior ventricular septal rupture are often accompanied by papillary muscle infarction or dysfunction, leading to mitral regurgitation. The diameter of the ventricular septal rupture can range from a few millimeters to as large as 3–4 cm. The edges of the rupture site are irregular, and the larger the rupture diameter, the greater the left-to-right shunt flow, resulting in more severe hemodynamic effects.
bubble_chart Clinical ManifestationsThe main clinical manifestation of ventricular septal rupture is the appearance of a rough holosystolic heart murmur several days to 2 weeks after myocardial infarction. The murmur is usually located at the lower left sternal border and may radiate to the axilla. Approximately half of the patients are accompanied by tremor. Some patients experience severe chest pain before the onset of the murmur. Ventricular septal rupture leads to an abrupt left-to-right shunt at the ventricular level. Patients with large perforations and significant shunting may rapidly develop acute heart failure, presenting with pale complexion, cold extremities, weak pulse, decreased blood pressure, reduced urine output, and dyspnea. About 50% of patients may die from heart failure and shock within a short period due to the severity of their condition.
bubble_chart Auxiliary Examination
Chest X-ray shows increased pulmonary vascular markings.
Electrocardiogram can indicate the location of myocardial infarction.
Right heart catheterization may reveal increased oxygen content at the ventricular level, with pulmonary blood flow often exceeding systemic blood flow by more than double. Pulmonary artery pressure and pulmonary capillary wedge pressure are elevated.
Selective left ventricular angiography helps determine the location and number of ventricular septal perforations, assess left ventricular function, and identify the presence and severity of mitral regurgitation, but it is not suitable for critically ill patients.
Selective coronary angiography helps evaluate the number and extent of coronary artery branch lesions and provides important information for determining whether concurrent coronary artery bypass grafting is necessary.
Echocardiography, pulsed Doppler ultrasound, and radionuclide myocardial scanning also aid in assessing the location and extent of myocardial infarction.bubble_chart Treatment Measures
Ventricular septal rupture causes abrupt hemodynamic changes, severely threatening the patient's life and often leading to death shortly after onset. After the onset, 25% of cases die within 24 hours, 50% within 1 week, and 70% within 2 weeks. Only 20% survive for more than 1 month after onset. The only treatment is surgical intervention to suture the rupture and correct the hemodynamic disorder. However, the timing of surgery involves weighing pros and cons, and there is considerable controversy.
After ventricular septal rupture, the ischemic necrotic myocardial tissue takes 6 to 8 weeks to complete the fibrous healing process. Surgery performed at this stage, when the condition is relatively stable and the fibrotic myocardial tissue around the rupture is more robust with better suture-holding capacity, has a higher success rate. However, most cases do not survive beyond 2 months after onset. Therefore, surgical treatment should be performed as early as possible. Yet, early surgery after onset carries a higher mortality rate. Brandt et al. (1979) summarized 105 cases: the early postoperative mortality rate was 41% for surgeries performed within 3 weeks of onset, compared to only 6% for surgeries performed after 3 weeks. Buckley et al. (1971) reported 5 cases operated within 10 days of onset, with 4 surviving postoperatively. Gaudiani et al., based on their experience with 43 cases, concluded that the patient's left ventricular functional status is a more critical factor influencing early postoperative mortality, with the highest mortality observed in patients presenting with cardiogenic shock before surgery. Additionally, advanced age and posterior ventricular septal rupture also increase surgical mortality.
Regarding the timing of surgical treatment, the current consensus is to tailor the approach based on the patient's condition. For some cases where ventricular septal rupture does not cause severe hemodynamic changes—manifested as no significant reduction in cardiac output, absence of cardiogenic shock, no symptoms of elevated pulmonary venous pressure, normal renal function, adequate urine output, and normal blood urea nitrogen and creatinine levels—close monitoring and continued medical treatment may be appropriate, delaying surgery until after 3 weeks post-onset when surgical mortality decreases. For most cases of ventricular septal rupture, however, abrupt hemodynamic changes after onset lead to rapid deterioration of circulatory function, presenting as cardiogenic shock, elevated pulmonary venous pressure, impaired renal function, and fluid imbalance. In such cases, surgical intervention must be performed as early as possible. Although early surgery after ventricular septal rupture carries a higher mortality rate, it remains the only option to save some patients' lives. If the condition progresses to grade III shock, affecting the central nervous system, or causing renal or other visceral organ failure, surgery should be considered contraindicated.For critically ill cases of ventricular septal rupture requiring urgent surgical intervention, insertion of a Swan-Ganz catheter is recommended. After confirming the diagnosis through pressure and blood oxygen measurements, intra-aortic balloon counterpulsation should be initiated immediately to temporarily improve cardiac output, prevent rapid deterioration, and support the patient during surgery.
Surgical procedure: Ventricular septal rupture repair requires cardiopulmonary bypass with hypothermia and various myocardial protection measures.
A midline incision is made on the anterior chest, the sternum is longitudinally split, the pericardium is incised, and the heart is exposed to identify the infarcted areas of the myocardium and ventricular septum. After systemic heparinization, a venous drainage catheter is placed in the right atrium or the superior and inferior vena cava, while an arterial perfusion catheter is inserted into the ascending aorta and connected to the heart-lung machine to initiate extracorporeal circulation. Ice-cold saline is used for
local profound cardiac hypothermia. A cross-clamp is placed on the ascending aorta, and cold cardioplegic solution is injected into the ascending aorta proximal to the clamp, allowing intracardiac procedures to commence.
For repairing a ventricular septal rupture secondary to myocardial infarction, a left ventricular incision is preferred over the right ventricular approach used for congenital ventricular septal defects. The right ventricular incision not only provides inadequate exposure of the ruptured septal area but also fails to properly address the paradoxical motion caused by left ventricular infarction or coexisting ventricular aneurysm. Additionally, the right ventricular incision injures healthy right ventricular myocardium and disrupts collateral circulation from branches of the right coronary artery, further compromising the blood supply to the left ventricular myocardium.
Brandt et al. and David et al. reported cases where ventricular septal rupture was repaired via a right ventricular incision, with postoperative left-to-right shunting recurrence rates of 38–41%. The most common site of ventricular septal rupture is the anterior septum near the apex, followed by the posterior septum, though it may also be confined to the apical region. When the rupture is limited to the apex, the infarcted area is smaller, making the repair technically simpler and yielding the best surgical outcomes. Conversely, repairing a posterior ventricular septal rupture poses the greatest technical challenge.
Apex Ventricular Septal Rupture Repair: Enter the left ventricular cavity through an incision in the myocardial infarction area at the apex of the left ventricle, expose the site of ventricular septal rupture, and remove the necrotic myocardial tissue in the diseased area of the ventricular septum as well as the infarcted myocardial tissue at the apex of the left and right ventricles. Use a Dacron patch to repair the ruptured area on the left ventricular side below the ventricular septum. Sutures should be placed in the normal ventricular septal tissue far from the rupture site, with a small patch placed on the right ventricular side as a backing. Then, suture the incisions at the apex of the left and right ventricles, with long strips of Dacron patches placed on both sides of the incisions, or use a patch to repair the apical incision. The sutures for the apical incision should pass through the lower part of the ventricular septal repair patch (Figure 1).

(1) Myocardial infarction area
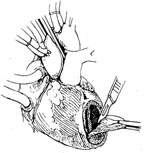
(2) Removal of infarcted myocardium at the apex and ventricular septum
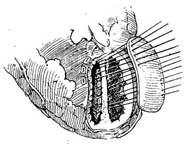
(3) Repair of the ventricular septum with a patch

(4) Schematic of ventricular septal repair
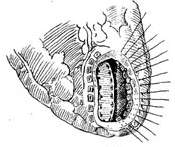
(5) Suturing the left ventricular apical incision

(6) Completion of suturing

(7) Repair of the apical incision with a patch

(8) Completion of the repair
Figure 1: Apex Ventricular Septal Infarction Repair
Anterior Ventricular Septal Rupture Repair: Make a left ventricular incision parallel to the anterior descending branch in the middle of the anterior wall myocardial infarction area, expose the ventricular septal rupture site, and remove the necrotic myocardial tissue from the ventricular septum and ventricular wall. Then, perform direct suturing or patch repair based on the size of the ventricular septal rupture. For smaller ruptures, the posterior edge of the ventricular septal rupture can be directly sutured to the anterior walls of the left and right ventricles using interrupted mattress sutures with pledgets. The sutures should be placed slightly away from the rupture, penetrating healthy myocardial tissue. For larger ruptures where direct suturing would create excessive tension, use a Dacron patch to repair the ventricular septal rupture, then suture the left ventricular incision (Figure 2).

(1) Left ventricular incision

(2) Removal of infarcted myocardial tissue
(3) Repair of ventricular septal rupture

(4) Completion of suturing

(5) Suturing the left ventricular incision
Figure 2 Repair of Perforation in Anterior Ventricular Septal Infarction
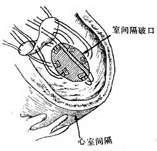
Repair of Posterior Ventricular Septal Perforation: Exposure of the posterior ventricular septal perforation is relatively difficult, and the procedure is technically challenging. After lifting and elevating the heart from the pericardial cavity, the infarcted area of the left ventricular posterior wall is incised to expose the ventricular septal perforation. If the perforation is small, the necrotic myocardial tissue of the ventricular septum and ventricular wall is excised, and the posterior edge of the perforation is intermittently sutured to the diaphragmatic surface of the right ventricular wall using pledgeted mattress sutures, followed by closure of the left ventricular incision.
For larger perforations, the ventricular septal defect requires repair with a Dacron patch. The patch is placed on the left ventricular side of the perforation, and another patch is used to repair the left ventricular incision (Figure 3).
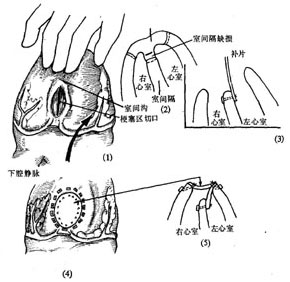
Figure 3: Repair of Posterior Ventricular Septal Infarction Perforation
(1) Elevate the heart and make an incision in the left ventricular posterior wall; (2) Excise the infarcted myocardial tissue; (3) Repair the ventricular septal perforation with a patch; (4) Close the left ventricular incision; (5) Schematic diagram of the suturing procedure
For cases requiring concomitant coronary artery bypass grafting, a segment of the great saphenous vein is harvested before initiating extracorporeal circulation. After completing the ventricular septal perforation repair, an end-to-side anastomosis is performed between the great saphenous vein and the coronary artery branch. Following removal of the aortic cross-clamp and cessation of extracorporeal circulation, the ascending aorta is partially clamped to perform the ascending aorta-great saphenous vein anastomosis.
Treatment Outcomes: In the past, the early mortality rate for surgical treatment of ischemic ventricular septal perforation was around 35%. Over the past 15 years, due to the adoption of the left ventricular incision approach and the use of intra-aortic balloon pump support before and after surgery to enhance cardiac output, the early surgical mortality rate has decreased to below 25%. The 5-year survival rate postoperatively is 75–89%, with significant improvement in cardiac function. Follow-up reveals that approximately 10–25% of patients still have residual left-to-right shunting at the ventricular level or recurrent rupture of the ventricular septal perforation after suturing. Patients with significant shunting may require reoperation.
Ventricular septal rupture needs to be differentiated from mitral insufficiency caused by papillary muscle infarction or rupture. Both conditions share similar medical history, clinical symptoms, and signs. However, acute mitral insufficiency often leads to clinical symptoms of pulmonary edema. The murmur it produces is typically located at the apex and radiates to the axilla, rarely accompanied by a tremor. Electrocardiogram examination often shows signs of posterolateral myocardial ischemia. Right heart catheterization reveals no left-to-right shunt at the ventricular level. Pulmonary capillary wedge pressure indicates elevated left atrial pressure, with the pressure curve displaying tall, sharp V waves.


