| disease | Congenital Radioulnar Synostosis |
Congenital radioulnar synostosis is a rare malformation characterized by the congenital fusion of the proximal radius and ulna, with the forearm fixed in a certain degree of pronation. Bilateral involvement occurs in 60% of cases, and there is no difference in incidence between males and females.
bubble_chart Etiology
This malformation exhibits dominant inheritance in some diseases involving the philtrum. During embryonic development, both the ulna and radius originate from mesodermal tissue. When the separation between the ulnar and radial cartilage rods fails to occur and ossifies, or when mesodermal tissue fills the space between the ulna and radius during the 5th day-night cycle of the embryo, radioulnar synostosis occurs. Type II radial head dislocation develops during the advanced stage of fetal development.
bubble_chart Pathological Changes
This deformity is generally classified into three types: Type I is true congenital radioulnar synostosis, where the proximal ends of the ulna and radius are fused together without cortical bone in between. The radial head may be fused with the ulna or completely absent (Figure 1A). The latter often affects both sides, with the radial shaft being curved, thicker, and longer than the ulna. The distal ends of the ulna and radius usually do not fuse. Type II involves posterior dislocation of the radial head, with the proximal end fused to the upper part of the ulnar shaft (Figure 1B). Type III is characterized by a connection between the ulna and radius via an interosseous ligament, which restricts forearm rotation. This type is not a true fusion but presents with consistent clinical manifestations.
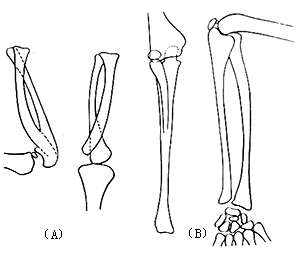
Figure 1 Congenital radioulnar synostosis
(A) Type I (B) Type II
bubble_chart Clinical Manifestations
There is no mobility between the radius and ulna, with the forearm fixed in a pronated position and loss of supination function. Extension of the elbow joint is partially restricted, while the wrist joint can move freely. The degree of impact on daily life depends on the fixed deformity position of the forearm. If only one side is affected, functional impairment is minimal. The affected forearm appears thinner and curved. Due to hypoplasia or anterior/posterior dislocation of the radial head, a localized depression can be observed at the normal position of the radial head.
The diagnosis can be made based on clinical manifestations and X-ray films.
bubble_chart Treatment Measures
The degree of deformity in each patient should be accurately assessed to determine whether surgical treatment is necessary. Generally, separation of the radioulnar synostosis is not recommended due to its often poor outcomes. If the fixed pronation deformity of the forearm is severe, exceeding 60°, a rotational osteotomy of the proximal third of the radius and ulna can be performed to position the forearm in a functional posture. The Kelikian rotational osteotomy is commonly used to achieve a certain range of forearm rotation. This method involves resection of the distal portion of the ulnar shaft combined with transfer of the flexor carpi ulnaris tendon to restore supination function, although the results are sometimes uncertain.


